
Transcript Pr Raoult YouTube video June 15, 2021 « Kill the messenger »
Translation : Citizen4Science from original transcript in French – video at bottom
Question: « Professor Didier Raoult, why do you call this program « Kill the messenger »? «
« Look I find that the IHU, which was created by this country, to deal with a lack of organizational skills in epidemics, and which has proven to be clearly functional, is subject to a series of attacks, including ad hominem attacks, against me, against my hair color, their length, that of my beard. I have been attacked, I will show you all the attacks that I have been subjected to by, who, the Medical Council of Physicians , justice that multiplies actions without stop and of which I will give you some elements, some discussions and I want to make you understand that, when one is there, it is that one has lost, when one cannot fight against the scientific reality because it ends up imposing itself, one has lost. Some journalists and politicians think that we can have a purely virtual victory, but not when we talk about medicine, because medicine is factual, it is not a digital object, as the GAFA would like to believe, no, it is humans, Afterwards, we can count those who are dead and those who are alive, and then, what you manage to impose in a country, but as Goebels managed to impose it in Germany, Goebels said: « If you repeat enough, with enough conviction, you can convince people that a square is a circle ». Yes, but in Germany, and for a certain time. That is propaganda. It does not stand the proof of time, because we are not the only ones, there are plenty of countries that use hydroxychloroquine, there are plenty of countries that do not care about our therapeutic results and the press can say what they want, life goes on. You see, and for example I will give you two lines that are ours, we, it happens that this institute has been brought by its size and its strategy to be the one with the greatest experience, by far, in this country and in Europe, we have all the data, we have millions of data. We have millions of data. The patients who have come to us, we have analyzed, as we go along, and whose data we release, we have 600 data per patient, and it so happens that here we have treated more than 30,000 people. So I don’t know if you multiply that by 600, you realize how much data we have.
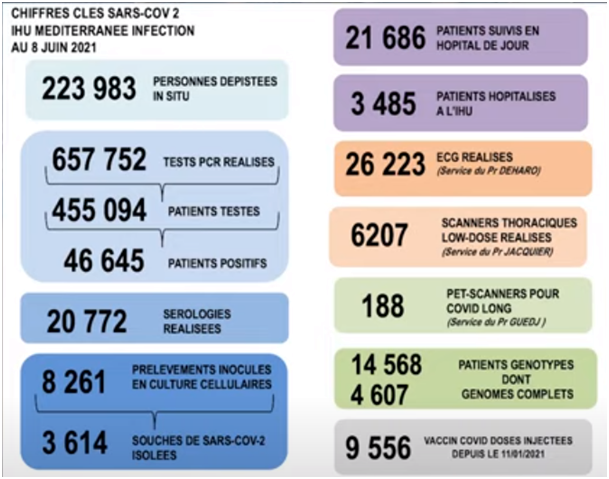
So it is not, we did not conduct a study with 4 given information fiddled with in a, in a pharmaceutical industry dispensary, it is real data with real patients. Besides, you know, people elsewhere think what they want, if you see what people in Marseille think about the IHU, I assure you that people know very well what happened. So, the first thing is that the number of data that we have, that we put once a week is considerable.
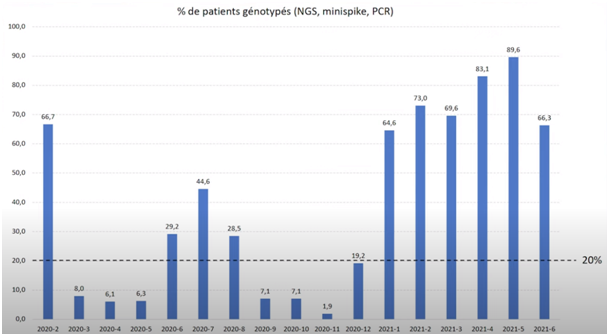
It is good, I am happy that people have realized, now, that it was necessary to make genotypes to know what was happening because it was not the same disease but several epidemics, so we made about 15,000. The idea is to make between 30 and 40,000 genotypes in order to have at least 80% of all the genotypes since the beginning of the people who passed through here, 40,000 in total, in order to try to understand all these cycles.
As people were worried about the risk of arrhythmia, i.e. cardiac disorders caused by hydroxychloroquine, we had 26,000 electrocardiograms checked by a professor of cardiology specialized in this field, only to learn, finally, 15 days ago that in the WHO website it was shown that the drug that caused arrhythmias was Remdesivir, 73% more arrhythmia with Remdesivir than with hydroxychloroquine, this did not make the rounds of the press because it goes against everything that people said but which was taken for granted. A drug that has been prescribed to billions of people for 70 years, if it was to give arhythmic disorders we would know it, while a drug that has never been prescribed on this scale, it is impossible to know in advance if it causes heart rhythm disorders, so this is the one we had to monitor. First of all, they chose a drug for which we did not know the risks, for which we did not know the consequences when it is given by infusion, because infusions always have consequences, thrombosis, infections, so you give pills, you give pills. So, while we did not know these elements plus the effects on kidney, the consequences in the medium to long term, that is to say, if you take a risk for an expected benefit, it is one thing, but when you know, with hydroxychloroquine that there is no risk, the nature was not the same.
To have succeeded in making people believe that hydroxychloroquine was a risky drug, it is one of the most extraordinary tricks of prestidigitation that I have seen in my life. But before people recognize that it was a conjuring trick, of course, it will take some time. Now, we have treated now, exactly, to date [searches in his notes] 16,900, about 17,000 people who could be evaluated with hydroxychloroquine+azithromycin, that is to say, a treatment of more than 3 days, that is what allows us to assess respiratory infections, and we have a mortality, including hospitalized, non-hospitalized, passed through the resuscitations, not passed through the resuscitations, of 0.8%. None died of cardiac events.
It is not true, it is a fantasy, it is not true, we already knew it was not true. But we confirm that it is a huge lie, it is not true. Okay, so there is a problem here, and if what we are saying is true, that is to say, what we are observing, and what many people are observing, and more and more in the world, and do not believe that it will stop, it will not be enough that there are 4 TV and 5 excited TV sets to stop the march of the world.
It is coming out everywhere at once, so when you give it early, you decrease, you divide by 4 the mortality, that’s what we have, what Matthieu Million published on 10,000 people, it is on our website. Jean-Christophe Lagier published on more than 2,000 people, people who were hospitalized, that is to say who were serious, that there was a 30% reduction in mortality compared to those who did not take it, because there were people who did not take it because the doctor was not convinced or because the patient did not want to, so we had a natural control group, we had, once we added that by age, and therefore, the mortality, in our case, the people who died and that we took care of, their mortality, their average age, of mortality, is 81 years. That is to say, these people are older than life expectancy. So we can’t imagine that this disease has decreased life expectancy, it was beyond life expectancy. So if everyone had been treated as we did, life expectancy would have increased, it is not possible! But then it is not arithmetic anymore, it is just arithmetic. So, of course, there were, there were some who had associated conditions who died younger, but as there are some who died at 93, 94, 100 years old, of course that compensated the average is 81 years old, 81 years old is more than the life expectancy in France, well, so, if we take care of the patients that we do everything that ended up being taken, anyway,
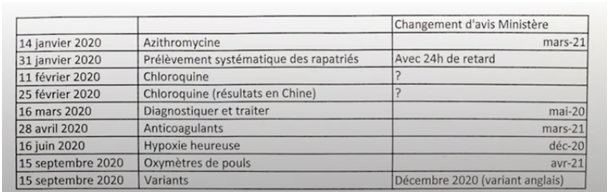
because I’m going to show you this document, all the elements that we put in place ended up being taken over by the State, after it was said that it was wrong, that wha we did was wrong, so then we gave them antibiotics, we tested them systematically, even though it was said that they shouldn’t be tested,
we now even have an email from Delfraissy who wrote to Fauci that in France we don’t have the means to test people, I don’t know who he asked if we could test people, but here we can see that he says that the whole policy was put in place based on the assumption that we could not test people, that was not true, we could test people, the proof is that we did it.
Afterwards, on the subject of chloroquine, I was threatened with death, I will talk about it later, I was insulted on all the TV studio sets without having heard the people who are supposed to defend research, the Minister of Research who never helped me, who never said a word to defend research, the president of INSERM who attacked me, the president of CNRS who attacked me, but what is this country in which we destroy the most famous researchers in the world, but are you crazy or what? Do you want to know what I did? You look at PubMed, you look at Massiliensis, Timonensis, that’s the name of two bacteria that I have provided, I have named 700 bacteria in my life and nobody has done that in the world, since we know bacteria, it would be easy to check, who do you think calls the bacteria Massiliensis and Timonensis then besides me.
It’s, all that, it’s easy to see. So we can’t afford in a situation like this to upset or try to destroy the people who have the most experience in this field. You’re crazy. Then when we finally, when I said, look, on March 16, we have to diagnose and treat, meanwhile, at the Ministry of Health they were saying: « No, stay home, do not see a doctor to take chloroquine ». It took a little time, then in the end, in May 2020, they finally said: « No no, doctors have to go see the sick, they have to be treated as sick », since when do you tell a doctor not to go see sick people? Since Greek antiquity we go to see sick people! Well, what is this story? We’re not going to invent now that we do not go to see the sick to cure the sick. What is this story of panic?
Then the anticoagulants, we were the first to put anticoagulants, we still think that, we still think that we manage to avoid one pulmonary embolism per week, then, we described the happy hypoxia, that is to say the fact that, people, contrary to what was recommended by the Ministry, That is to say, to go to the doctor when you are out of breath, in reality you don’t realize that you have no more oxygen and that you have to measure it, we wrote that from June, from June 2020 and afterwards we recommended the purchase of, in pharmacies, capacities to measure yourself your hypoxia, with the pulse oximeter, and then we started to, to discuss, us, the variants, from August, during the time, during this time, everybody was laughing at us saying that there were no variants and the French never understood that the biggest variant and the first one had been, there had been some in France, And they started to talk about variants when the English said that there was a variant, that is to say that the denial of all that was found in this country, it is something that was absolutely spectacular, that is something that is the questioning of the very knowledge that is something that is extremely serious. And of course, I don’t imagine that, considering the way people are moving forward, the more we will be right, the more we will be annoyed. Because to admit that we are wrong is something that is extremely costly. And when being wrong, if the figures we have are confirmed, it means that there were 25% more deaths, it’s a funny mistake.
So, it’s not going to stop, we’re not going to stop poisoning us. Don’t get your hopes up, we’re going to be gone for a while, because what I’m saying, if we end up agreeing, is that if we had done what I was advising the Scientific council, and the scientific council and all the others, to quickly, at least try, to have at least one trial like ours hydroxychloroquine plus azithromycin for almost a year and a half, but rather than talking about it and saying that it doesn’t work and that I keep saying that it does work, we should have tried it, the people who have tried it, there, in the resuscitations, in New Jersey, they have achieved results comparable to ours. So it was enough to try. When we submitted requests for authorization to carry out this treatment, they were rejected, they were rejected by people who were general practitioners and who told us that we didn’t know how to do research, well, that is bordering on insulting, it’s embarrassing. «
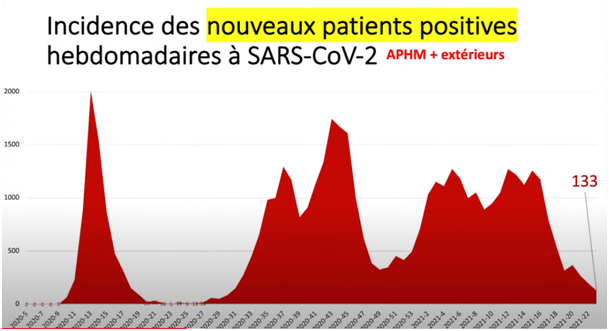
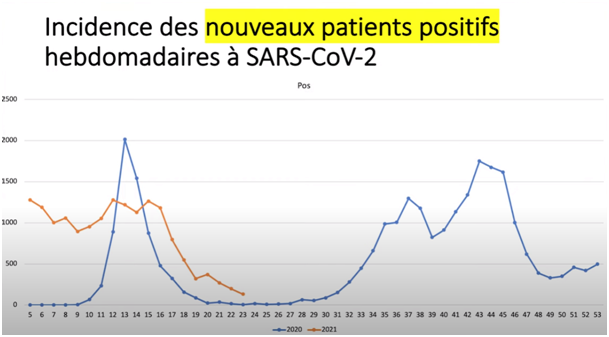
Question: « Where are we now in the epidemic?
Right now, the epidemic is like this, that is, the number of cases is decreasing. You see we are, it is quite low, now, there we had 133 next week, we have less than a dozen per day, we have about 20% in those who are vaccinated, we don’t know too much what is the proportion that will increase, then we will see the number of English variants decrease dramatically we have some Indian variants that are currently rising we will see what comes up and you, if you compare the epidemic to the one we had last year, you can see that it is the same pattern, the number of cases decreases and then, at the end of the spring, at the beginning of the summer, we can see that it follows the same seasonal cycle.
Then, what it will become, well I will show you this, you will not be able to understand what it is, but it’s the data we have on mortality in all the countries of the world.
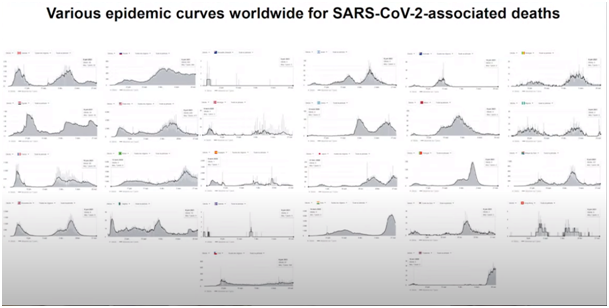
See if someone explains to you who could make a model out of this, you can tell him he is a crook, right. No one could have guessed why it would happen like this here. Some things have two backs, some things have only one back, one thing we understand is that the islands that closed had only one peak. So it’s not the disease that rebounds, it’s the fact that there is a second epidemic with variants that come from outside. And where do these variants come from? Now we know that these variants come from animal sources. From what animal source? Essentially from what we, a family called mustelids in which there are minks, okay, there is a huge source with minks, but also with wild mustelids, badgers, civets, this is what we had already seen with the, the first SARS epidemic that went from bats to civets to humans and so this, this means that very often, these new variants are likely to come from places where there are farms of susceptible animals and this group of mustelids has much more sensitivity to these viruses and so very often, these RNA viruses pass, so the biggest reservoir of RNA viruses is bats, in a bat cave, you can have several millions of bats rubbing each other, and so the transmissibility of viruses is absolutely hallucinating, you have absolutely colossal reservoirs of viruses and from time to time there are mustelids which are carnivores that eat a bat, that catch the virus, or the bats urinate in the places in which the mustelids pass, they catch them and by chance, there is a mustelid that is sensitive and this mustelid has capacity to transmit something to the man rather easily. To fix ideas, ferret, which is a mustelid, is the experimental animal that has been the most used for all the human respiratory infections with RNA virus, so that explains you that ferret can transmit it to you that between the ferret and us the communication of the viruses is extremely important as with all the mustelids, that is it. So, we have to monitor, probably close all the mink farms at the moment, to, I don’t know, make synthetic fur, or I don’t know what to do, but in any case it’s a, these intensive mink farms represent an unquestionable danger for humanity, we will have to take a sanction on that, that’s it. So that’s the evolutionary situation, the therapeutic situation is there, you see.
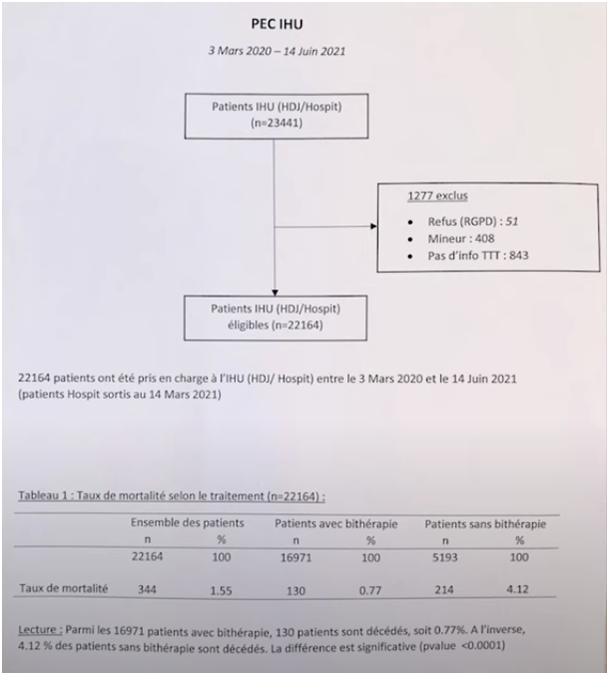
Here we have a recent update up to June 14, and you can see that the patients who were treated here, 23,000 patients, 22,000 were treated, and you can see that the mortality rate among people who were treated with dual therapy is 0.77 compared to patients who were not treated, which is 4.12. So we have 5 times less patients who have died among those who had treatment than among those who did not have treatment, So we have 5 times less patients who died among those who had treatment than among those who did not have treatment, and when we do propensity scores, that is to say, we make combinations with age and sex, we continue to see a difference that is significant.
I treated as many patients as you out of 22,000 and hydroxychloroquine killed three times more, I don’t think anything because I don’t know the work of others, I examine the people who have come here and we look at them and as we don’t hide the deaths, these are deaths reported by INSEE, we don’t hide them, everyone can go and check all the data we have on a site that accessible to everyone, we share everything because we have nothing to hide. So, that is the major element. So uf you have the elements that we saw, you can see that we had people who were only positive, not all of them came to be treated in the day hospital, some were hospitalized.
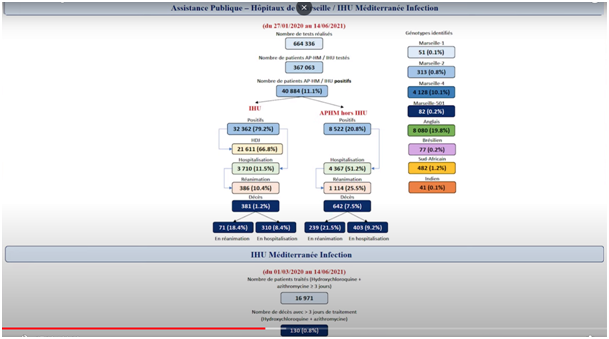
And then inside there were people who did not want, there were doctors who did not want to use this treatment, there were patients who did not want to receive it, There were others who were contraindicated, so not 100% of the people were treated, and this is good for us, because it allows us to monitor whether things are going better when people are taking or not taking the drug.
If we adjust for age, here you have the results for the 16,977 people who have been treated to date, and 0.8% of them have died, including those who went through hospital, resuscitation unit, etc. So that’s the situation we have, this situation is currently reinforced by a latest paper in pre-print, so I told you what we had on mortality, among patients in day hospital, among hospitalized patients, that is the mortality in intensive care.
You see, this is New Jersey, and what they find is that if you give a good dose, because it is a problem that there is in the literature, it’s that including people who have done studies in France, in England, it’s that they were giving anything. Treatment. They adjusted the concentration of antibiotics by dosing, as we did, we did several thousand dosages, before stabilizing the thing, and I based my experience on more than 4,000 patients dosing hydroxychloroquine, so we knew how much to give, so we had doses that were effective.
If we use effective doses, well, they multiply by three the chance of survival in patients who are critically ill, where there is a mortality rate of 72%. So, whether it’s very early, in the middle or very late, in all the serious studies, and which have, which are done in people who have been diagnosed for good, not, because there are some, some works which are published in the New England or in the Lancet by Solidarity, Recovery, what is supposed to be the reference studies where they have not, there are people who have not even had the diagnostic test who are included, we don’t even know what they have, some of them know that they didn’t even have it.
In the UK, 10% of people had negative tests. And they are included in the analysis, it is medicine from I don’t know, I don’t know where it comes from, who taught medicine to these people? A diagnosis in infectious diseases requires an infectious disease test. Otherwise it’s not that. It’s, we don’t know what it is. You don’t diagnose an infectious disease by saying I think that’s it. That’s what they did in the 19th century, it’s not true.
So it is unheard of what happened in the trials, it defies understanding, that is to say, to use the method, if you will, on patients who are not patients of the disease, if you will, it reaches a delirium that was, well, I didn’t think that I would ever see that, one day, I didn’t think that it was possible. In the beginning, we were especially concerned about genotyping, from the moment we saw that it was starting again in June or July, because I didn’t believe in this story of rebound, I thought it was a variant and so that’s what we found.
At the time, you remember, nobody believed us, that it was a variant, that [inaudible] nonsense [inaudible] to say so much nonsense, and people heard about the new variant from the moment when the English said that it was a new variant, see, when we say that nobody is a prophet in his country but finally we were the first in the world!
It was refused in all newspapers to which we sent it, we ended up sending it because people did not want to accept that there were variants. It was refused in Nature, it was refused in, in 3 newspapers, all of them, then afterwards, we put it, anyway, we put it online so we were the first to describe that there were variants, and these variants, there were 2 successive ones, one in Marseille, one in Mayenne, which was just next to the mink outbreak of Eure et Loir, very quickly, I, I warned the authorities that, the authorities that I thought that it was mink. I wondered if it was mink from Denmark because I didn’t know that there was mink in Eure-et-Loir, and as this Scientific council lacked all the people who, all the people who had scientific notions, there was not a single veterinarian, of course, nobody knew, in this scientific council that there were mink farms. So, well, I have a veterinarian here, everyone who works on infectious diseases has a veterinarian with him to work with, because, the animal sources, the zoonoses, that’s it, it wasn’t necessary because they knew, by dint of working on AIDS they knew what was happening in animals, well that’s not serious, that’s not how we work. We don’t just work with people who make prophecies and then people who worked on the AIDS trials.
I mean, it is not, we can’t deal with an epidemic like that, it’s not true. And then, so what we saw, we saw a first, a first, a first variant that was here, that disappeared that really didn’t come from a boat from the Maghreb, and then the second variant that appeared here at the same time as in Occitania (region of South France) and then it appeared in Denmark, that’s what put us, moreover, the flea in the ear because there was a huge epidemic of, among minks in Denmark where they slaughtered 17 million minks and then we thought that it could come from there and then we learned that there was a mink in Eure-et-Loir and it took me 3 months and a half to have the result of the sequence that had started to be done in November, 15 because I was sure that it was that one. And it was hidden from me for three and a half months [laughs]. So I finally got it and when I got it, knock, it fell in the middle of the 4th and so you see, what happened, we, with everything we sequenced, here in France, you see
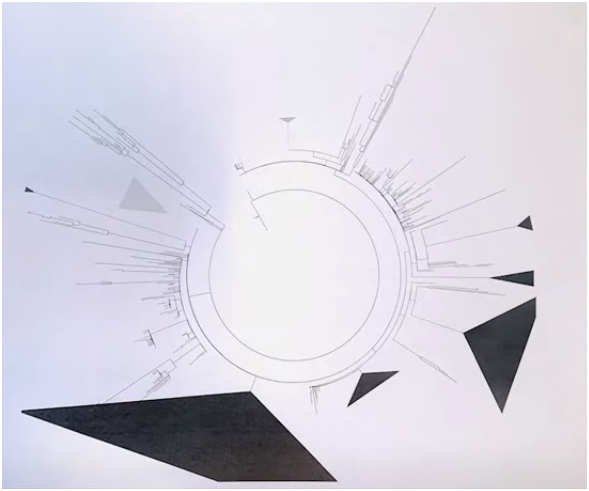
The biggest one, the huge one, is the 4, so, I was told that it’s not a variant, that comes from mink, it’s this one, this is the one whose existence was denied for I don’t know, 6 months, even now, I don’t know, I think there are still people who say no, it’s not a variant, it’s a standard virus, but I don’t know if you can see that it’s a phylogenetic tree, it was not me who made the tree, It’s the machine that made, see, this is the English variant and this is the, the variant 4, it’s monstrous what it gave if you see like this what it is, it is good, that if we take it from GISAID, if you see, that is to say, where all the stuff is deposited, you see that it is made in France that is to say that we can’t say that we did not do anything in this epidemic.
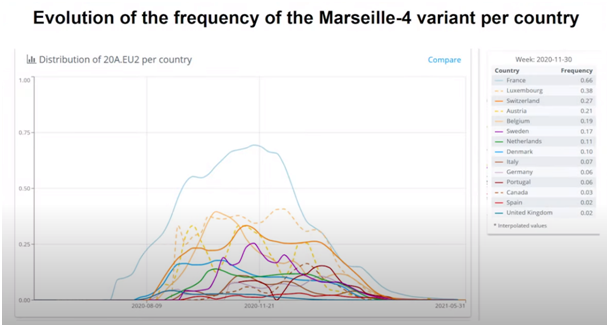
We did something, we did the virus that was the most epidemic of all Europe probably thanks to our minks. See all the lines, there, the line at the top, it is France, it’s us, and it is probably the most deadly of all the Covid epidemics that we have. That’s it, deadlier than Wuhan and deadlier with UK’s.
So, it is all about working, succeeding, doing things, with the risk that if you work, if you explain what you’ve done, there is an old Greek and Latin saying that you have to kill the bearer of bad news, which the English translate as « Kill the messenger », and so, there is a kind of relentlessness on us who provide the only exploitable data that we have in this country, the only data that are now used by the Ministry of Health to treat people. We have been harassed in a way that surprises me, God knows it is difficult to surprise me, so the first time I spoke about what was happening in China, I was accused of spreading fake news.
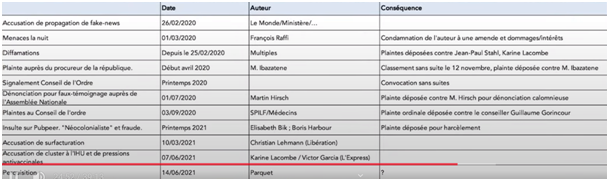
Censored on Facebook by Le Monde (french newspaper), the Ministry, then I was threatened with death by the Professor of Infectious Diseases who received the most money from Gilead, and finally from the pharmaceutical industry who was fined and ordered to pay damages. Then I had multiple defamations on all the television sets so I filed a complaint against Jean-Paul Stahl and Karine Lacombe who were among the most insulting. Including Karine Lacombe, who claimed that I had several complaints against me for false testimony, I, it’s, really, then, there is a complaint here to the Public Prosecutor by Mr. Bizi Ibazatene who is someone who is a freelancer for the pharmaceutical industry which was filed without any follow-up of course I filed a complaint against him, I am bothered by a complaint to the Public Prosecutor in Marseille, then I had a report from, to the Council of Physicians, in spring 2020, to ask me to stop expressing myself on the science I was practicing, I told them that the freedom of expression of academics in this country is free since the Middle Ages, that it was suppressed during the French Revolution, and that it is protected by the Constitution and by the European Court of Justice.
So if people want to prevent me from expressing myself it will go very, very far, but they will be condemned because there is already a decree that I have already shown, of, of the constitutional court we cannot prevent, we have a freedom of speech in general and more particularly when you are, an academic, we have not only the right to express ourselves but the Constitutional Council explains that we have the duty to express what we know because we are paid to generate knowledge and therefore we have to diffuse it.
Okay, so, if I were prevented from disseminating my knowledge it would violate the very rule of my job, which is to generate knowledge and to communicate it, okay. So, of course there’s no way I’m going to let that happen. I won’t let it happen. Then the denunciation of false testimony to the National Assembly by Mr. Martin Hirsch, who wrote to the National Assembly to say that I had given false testimony, because he didn’t even know the figures for his own hospital. And when we gave him the figures from his own hospital at the National Assembly, he didn’t know what to say, because the figures, of course, you can’t imagine.
I am not a television man, I am a figures man, I am a scientist, I am a scientist, what I say is based on data for which I have documents and reality and so Mr. Hirsch did not know how many people were dying in his hospital but it so happens that I had an internal document from the Assistance Publique des Hôpitaux de Marseille that I passed on and in front of which he stammered saying no, no, it was at the beginning but not at the end, so, uh, he quickly calmed down. Because you can talk nonsense on television but you have to be careful when you, you take decisions of this order, it is very serious to accuse someone of perjury at the National Assembly, say, I had taken an oath, I am a reasonable man who knows when he takes an oath and I do not see why I would lie before an institution of this nature that I respect. I am a republican after all.
It’s shameful to say things. I hope that it will be relocated because I fear that Mr. Hirsch has too many friends in Paris. So, I will try to have it relocated to another city, so that we can look objectively at whether Mr. Hirsch has the right to write to the National Assembly that I gave false testimony and whether he cannot be sued for slanderous denunciation, which means that anyone can say anything before the highest authorities of the Republic, and this is shameful. Because we are Mr. Hirsch, we have the right to, to, to say that, and it’s unimaginable. Then I was subjected to an absolutely unheard of assault on PubPeer by Madame Bik, and Mr. Barbour with a whole series of insults, because, there are 40 papers on which they put that our work was a neo-colonialist work, we who have received and trained 1000 students who come from the South. And we have what, the director of INSERM and CNRS who say: « Wait, this is a legitimate scientific debate, you should not sue these people for defamation ».
Wait, if that is not defamation, then what is the right to insult people by saying I am a scientist, I am insulting you because you are a scientist, but what, everyone has gone crazy or I’m the one who is crazy, people are crazy, what, there is no other way to do it…
There are people who have a lot of connections, a lot of networks, I do not have any networks because I am here and I work, so I work, I do not have any networks, I do not have the time, so, but people who spend their lives in Paris going to see each other, the editors, the newspapers, the things and everything, saying look I am a poor victim, they say that to people who do not read anything, who do not know what they are talking about, and who end up signing petitions or things saying wait, let’s let everyone do their job when people are insulted and defamed and harassed, that becomes the role of the Justice.
I’m not going to argue with someone who explains to me that I am a liar, a thief, a cheat, wait, I have got other things to do, at the end of the day when you go too far, if it is one time that goes by, I get so many of them, I do not even pay attention, but when it goes too far it becomes the role of Justice and when you want to be Zorro you have to have a minimum of credibility. You cannot be Zorro if you do not know what you are talking about.
So Madame Bik is talking nonsense. What she is saying is nonsense. It is personal hatred. Well, look, that’s what a lawsuit is about, and it cannot be settled any other way. I am very amused because at the CNRS, if you like, I had a little twinge in my heart. At the CNRS, there was the acting director of CNRS and the director of Life sciences who were attacked very, very violently by PubPeer a few years ago. One was immediately ostracized, relieved of her duties, she had a depression.
She had an extremely bad experience, the other one was, gave her file to her university which considered that there was nothing in her file and in the accusations made against her by PubPeer which led to changes in the results and its interpretation and therefore there was no fraud. All right. I felt sorry for her because she was a particularly hostile assistant director at the time. So there you go.
So you see, one can be stupid at times. You can lose your lucidity when people annoy you, when they have annoyed you, you can rejoice in their misfortune even when these misfortunes are silly. Okay, I deeply regret it. I apologize to him, I have never expressed this publicly, but I apologize to him because as long as we are in the situation of the, of the, we don’t live it exactly like when we see it in others. But at the time, the director of CNRS made a statement with his hand on his heart saying that the people of PubPeer were thugs and that denouncing anonymously was the way of the crows, and now, as it is me, they change their mind, they think that it is very good, we put anonymous denunciations without even knowing what we are talking about.
So these people are not reliable, these people have no soul. I don’t know what they have, but it is a problem of changing your mind by saying listen, now there is a mailbox where you can put anonymous messages insulting people that nobody checks and that’s fine, while we said two years before, listen, it is scandalous, so you have to have a little consistency.
Now, afterwards, Mrs. Karine Lacombe and a Mr. Garcia (journalist « L’Express » newspaper), whom I do not know, told us that we had a cluster case at the IHU and that we had inter-vaccinal pressures I don’t know what this is about, it’s nonsense, I do not know what it is about, the cases that we had, they are strictly parallel I can show you the pressure of, of the environment, that is to say that when we receive 2,000 positive people per day, there are more cases than when we receive 100, it is exactly parallel, it is relative risks, it is to protect ourselves, we have relatively few cases, we are around 30% of nosocomial infections in the care personnel, we don’t have any in the technical staff, we don’t have any in the students, so it’s not in the lecture halls that they catch it and those who have the most with the care staff are the administrative staff at the reception, that’s it, those are the ones who are the most exposed and it’s between 20 and 30% of the people who have it like, It’s between 20 and 30% of the people who have it, rather less than what we see in all the people who have received a lot of people from Covid, so all this is just, it’s once again just maliciousness.
As for the last search, it was suggested by an attack on the IRD a few years ago, I will tell you one thing, we have to be careful in this country to spare the honor of our country.
Yolande Obadia, who is the president of this foundation (IHU Marseille) is a woman who has been working here voluntarily for 11 years. For 11 years, she has not asked for a penny, to help us, to organize ourselves, there is a quantity of things that she knows how to do that I don’t know how to do because she is more diplomatic because she doesn’t have the same perceptions of things, it is an association without which our foundation could not have become what it is. She is someone for whom I have a very deep respect, who does not put herself forward, but this foundation could not be what it is if she had not been there and it is unheard of not to reward this woman at the level she should be.
If among all these people who got the Legion of Honor because they prescribed drugs for Gilead instead, we would have done something reasonable. Because people of this nature, who spend an important part of their life, entirely voluntary without expenses of function uh to take care of the general interest, and to resist the inconveniences to which it is subjected to be able to make service to their country, from time to time, this country is not serious.
We have to pay tribute to them and we have to respect what she does because she helps us a lot and she will continue.
I hope with all my heart, to help us because we would never have been able to take care of all these patients if she had not organized the whole recall of the patients, I remind you that we had thousands of positive people and that we had to call them back to give them appointments to offer them treatment. It was Yolande who organized this with 200 volunteers. And now we are facing another mountain that we will have to take care of, which is now our next duty, which is to take care of the post-covid people where we estimate that there are between 10 and 20% of people who need exploration with Covid, with cerebral damage, with aortic damage that we don’t know what will happen to them, perhaps with risks of cancer, okay, we will have to contact them, those who are sick.
We have, we have done, with, I recommend you to look at the preliminary work that was presented by Carlo Linda on our site, it is probably the largest in the world, we have done more PET scans, that is to say, examinations of brain function and metabolic disorders of the entire body, than any team in the world.
We are beginning to have data that are very important. We need to think about therapeutic management: chloroquine we have to try to analyze whether a certain number of these late manifestations were prevented by the treatments, in particular by hydroxychloroquine, because it seems to me that there is a tendency to avoid post-covid in people who have been treated.
This woman should be thanked, congratulated, and not harassed as being a collateral damage of the irritations that I cause by doing my job. Okay, I’m tough, and I can say that I despise most of the people who attack me, not everyone is like me, so focus the fire on me, I get a kick out of it, spare the people who work with us who do not stop, who give their souls, their time, most of the time without receiving, in any case without receiving a penny more, the others, the ones who are civil servants and the ones who are volunteers.
That’s all we have here. No one is making any money. So now we have to respect them, treat them right, okay, and we have to recognize that the quality of their work is exceptional and it’s these people that the Republic should thank.
« Thank you very much ».